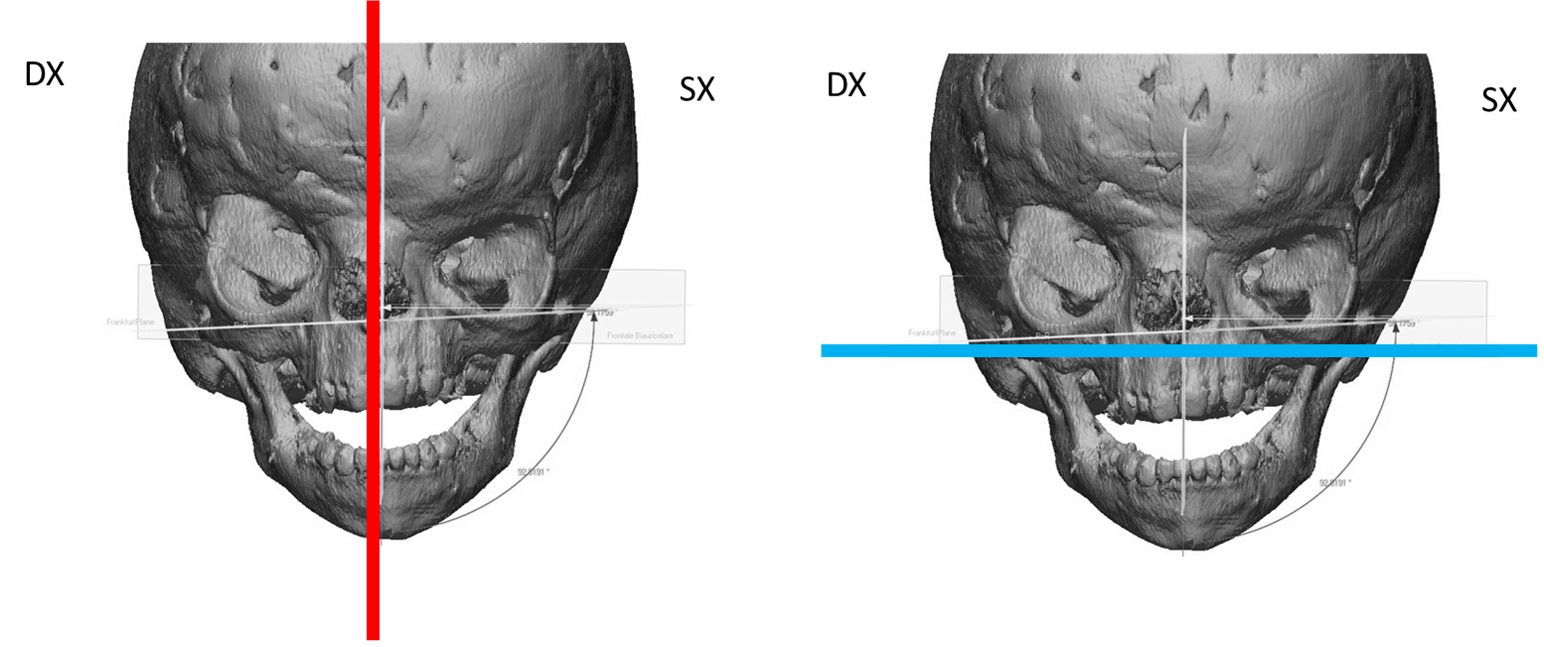
The possibility offered by 3D techniques to simulate the final result of the operation before performing it are also applicable to the treatment of hypertelorism. The images that we show of 3D reconstructions and preoperative studies refer to the case of a patient suffering from hypertelorism that had already undergone surgery in the past for the correction of a right anterior plagiocephaly. The patient presented with an important dysmorphism of the craniofacial region (Figure 1).
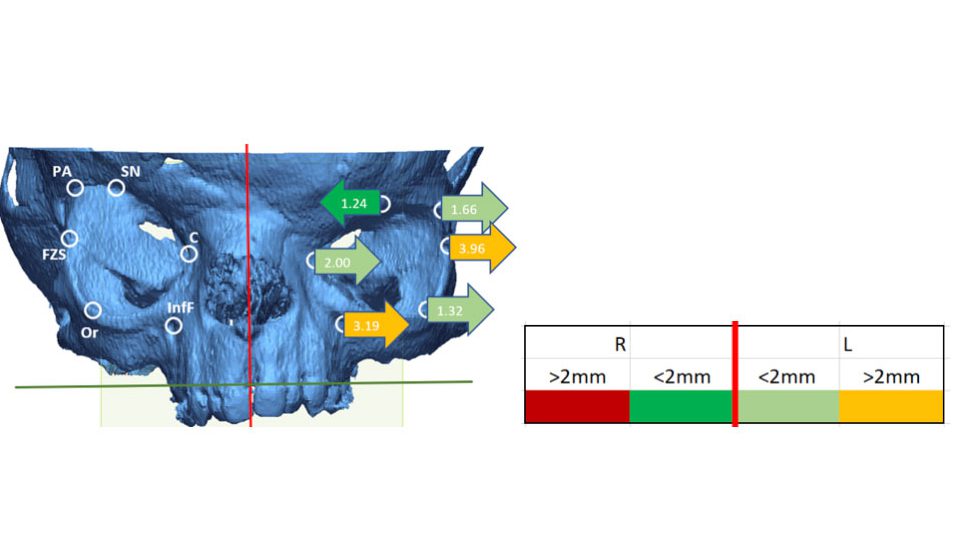
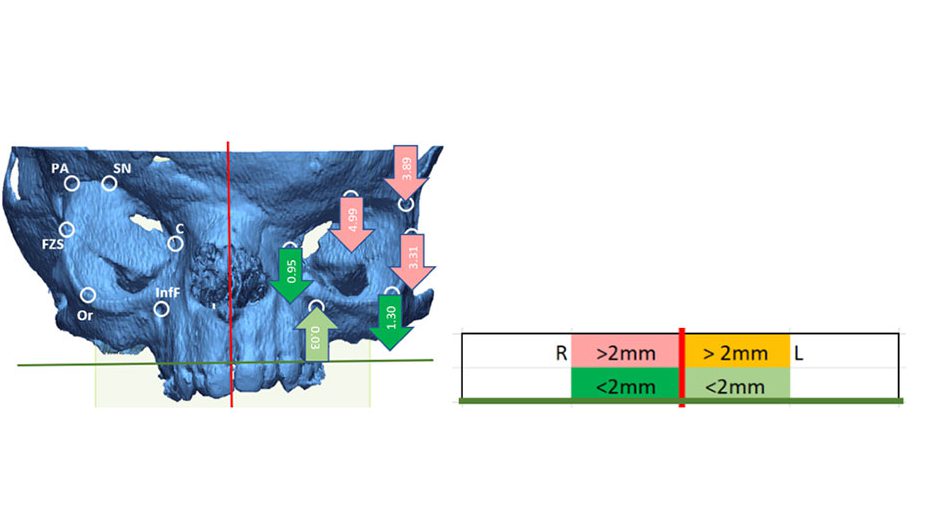
The cephalometric study based on the anatomical landmarks around the orbits showed important asymmetries even greater than 2 mm. The analysis of the asymmetry measurements made considering the anatomical landmarks of the left orbit compared to the corresponding ones of the right orbit allowed a much more precise diagnosis of the geometry of the patient’s skull (Figures 2 – 4).
Depending on the plane of view considered, it is possible to establish the exact geometric condition of the orbits in terms of symmetry.
Direction perpendicular to the median sagittal plane (Figure 2): The left orbit is shifted laterally with respect to the right orbit.
Direction perpendicular to the transverse plane (Figura 3): The topmost points of the left orbit are up to 5 mm lower than the corresponding points of the right orbit. The lower points of the right orbit are on the same horizontal line.
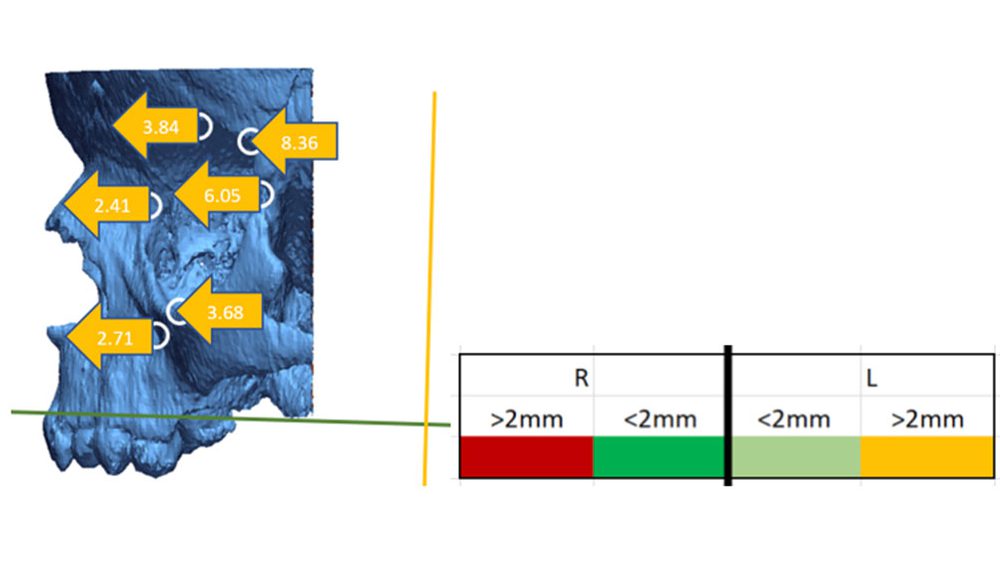
Direction perpendicular to the frontal plane (Figure 4): all the anatomical landmarks of the left orbit are shifted quite forward than those of the right orbit (difference greater than 2 mm).
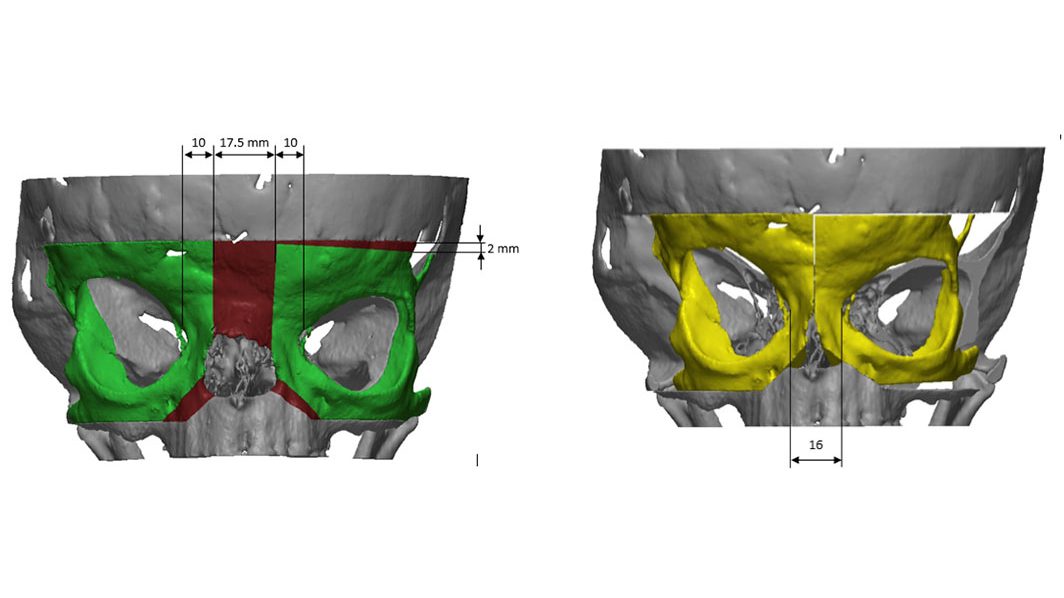
The results of the cephalometric analysis made it possible to define the displacements for symmetrical repositioning of the orbits. These displacements are very complex, involving translations and rotations in space of very different entities.
Given the complexity of the case and the strong measured asymmetries, the necessary osteotomies and the subsequent repositioning of the orbits were therefore simulated pre-operatively (Figure 5). Patient-specific templates were then designed to guide the osteotomies and the subsequent symmetrical positioning of the bone segments. This allows a result as close as possible to that simulated to be obtained, minimizing asymmetries and maximizing both aesthetic and functional results.